A Broken Chain
At the end of March, shortages of ventilators, surgical masks, and other personal protective equipment (PPE)—not to mention panic-induced runs on items from toilet paper and hand sanitizer to eggs and flour—were giving Americans a crash course on supply chain management.
At the end of March, shortages of ventilators, surgical masks, and other personal protective equipment (PPE)—not to mention panic-induced runs on items from toilet paper and hand sanitizer to eggs and flour—were giving Americans a crash course on supply chain management. Supply chain management—formerly a somewhat obscure economic concept—started to become a topic of public concern as daily newscasts covered shortages and tallied scarce items delivered to medical facilities. The supply chain, as most Americans soon discovered, affects every aspect of our daily life, from what we eat to what we can buy to what critically needed supplies are available in times of crisis.
By April, with COVID-19 affecting most of the world, global
and local supply chains and distribution efforts had begun
to creak. On April 13, the New York Times reported that the
nation’s food supply chain, composed of the farmers and
distributors and packagers and retailers who fill our grocery
stores, was showing strain.
For instance, dairy operations that sold to commercial
vendors throughout the country were dumping milk
because, with restaurants and schools closed, much of
their customer base was gone. Distribution and packaging
challenges made donating the milk very difficult, even while
many in the country were going hungry. CNN reported the
Dairy Farmers of American estimated between 2.7 million
and 3.7 million gallons of U.S. milk could be dumped a day.
Vegetable farmers were also being forced to plow under
thousands of acres of ready-to-harvest crops, due to shuttered restaurants and a dearth of other markets to absorb
production. Farms also lacked workers to pick the crops.
“For some Minnesota growers, restaurants were 90 to
100 percent of their market,” says Constance Carlson, the
codirector of Statewide Sustainable Agriculture and Food
Systems at the U of M’s Extension Regional Sustainable
Development Partnerships (RSDP). RSDP is collaborating
with the Minnesota Department of Agriculture and the
Minnesota Grocers Association to help growers tap into
emergency market channels.
Even with that support, it’s a devastating situation.
“Agriculture moves slower than the consumer response to
a pandemic,” says Sarah Swan Ray, a supply chain development specialist at RSDP, who focuses on more vulnerable
growers, including Latino and Hmong farmers. “And the
farmer gets a bad reputation. This is a travesty.”
Some growers will decide not to plant this year, reasoning
that a financial loss before production is preferable to paying
labor costs for goods that may never get to market. Others
may move ahead with planting and hope for the best.
It will be difficult, even in a best-case scenario, for growers
to donate unsold produce. “They would have to spend
money to harvest, clean, package, and move it off the farm,”
explains Swan, who notes that many farmers operate on
such thin margins that even in good times they don’t pay
themselves a salary. “If a crack team of emergency response produce harvesters could take care of the labor, I think farm
-
ers would be happy to [donate their products].”

Likewise, it will be challenging for many growers to
pivot to alternative options, including farmer’s markets or
community sponsored agriculture (CSA), where consumers
buy local, seasonal food directly from farmers. Social
distancing at farmers markets will reduce capacity; selling
directly to consumers puts farmers at risk for getting sick.
Ray says that older growers and more traditional com
-
munities
—including many Hmong farmers
—are less able to
adapt to touchless systems, such as ordering on websites
or paying with Venmo or other cash-free options. While she
and other experts see potential in these new ways of doing
business, they note that it’s hard to implement new systems
in the middle of the growing season.
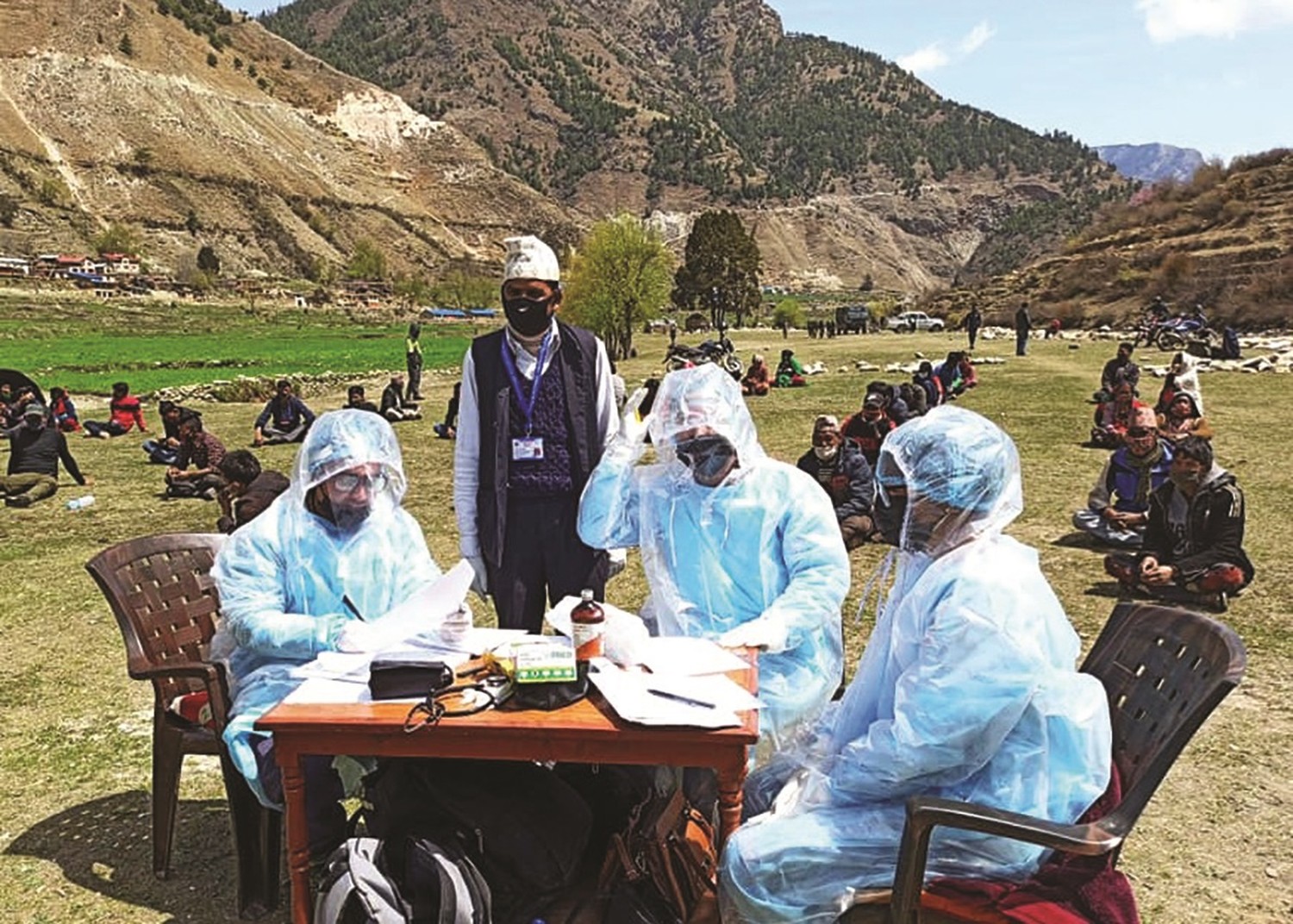
Another problem affecting animal farmers came into
sharp focus in mid-April, when the first of the nation’s
meat processing plants, owned by Smithfield Foods in
Sioux Falls, South Dakota, was forced to temporarily close
because so many of its workers were ill. This was followed
quickly by the COVID-19-related closure of a number of other meat processing plants. That left a number of farmers, particularly in Minnesota, without a place to sell animals
as they reached market weight. Some farmers were forced
to cull young animals because they lacked space to raise
them, given that their lots were already full.
Some worry that these distribution issues could continue
to affect the availability and price of meat months from now.
In response, on April 28, President Trump signed an executive order under the Defense Production Act, mandating
that meat-processing plants remain open as part of the
nation’s critical infrastructure.
Medical Matters
A Bitter Pill
Could COVID-19 affect the
supply chain of life-saving
drugs in the United States?
The Resilient Drug Supply Project is
an initiative of the U of M’s Center
for Infectious Disease Research
and Policy (CIDRAP) that maps the
supply chain
—from raw materials
to patients
—of critical medicines
used in the United States health care
system. In late March, preliminary
findings from CIDRAP identified
156 drugs that are critical to keeping
Americans alive, noting many
of these drugs are sourced or
manufactured in countries that have
experienced production shutdowns,
including China, India, and Italy.
However, because drug
manufacturers aren’t required by
law to disclose to the Food and Drug
Administration or the general public
where their products are made,
it’s difficult to estimate the precise
health risk to Americans due to
possible supply chain disruptions.
As a result, CIDRAP publicly called
upon pharmaceutical companies,
their suppliers, and manufacturers
to disclose supply chain details on
these critical drugs.
“This is life and death, and the public needs to know where their drugs come from and be assured they will always be available in a timely manner,” according to Stephen W. Schondelmeyer, coprincipal investigator of the project and professor in the College of Pharmacy at the University; Century Mortar Club Endowed Chair in Pharmaceutical Management & Economics; and director of the PRIME Institute, an independent and global research, education, and consulting organization that studies economic and policy issues to help improve access to pharmaceuticals and pharmaceutical services.
As experts scrambled to address those issues, other supply
chain problems were also becoming apparent: Entities such
as the U of M’s Center for Infectious Disease Research and
Policy (CIDRAP) warned it was possible the key ingredients
for drugs could be disrupted by the global pandemic in
coming months (see sidebar at right).
Perhaps most critically, as experts said additional testing
for COVID-19 is needed to safely reopen the country, false
starts hampered those efforts. Supply chain issues slowed
the rollout because tests didn’t work or lacked the critical
supplies necessary to properly conduct them.
By late March, the U of M announced it had created
an on-site COVID-19 testing location, but tests would be
limited to just 64 per day because of the nationwide
shortage of testing and extraction supplies. “If we’re
planning for a 30-day window of testing, assuming that
we receive no other supplies, we can do 64 tests per
day for the next 30 days,” Sophia Yohe, M.D., associate
professor in the Department of Laboratory Medicine and
Pathology, said at the time.
To help circumvent those issues, by mid-April the U of M,
the Mayo Clinic, and the Minnesota Department of Health
had developed tests to detect antibodies in people who suspected they had had COVID-19 and to test for active infections.
The lab of Marc Jenkins, (B.S. ’80) a Regents and
Distinguished McKnight University professor at the
medical school and director of the Center for Immunology,
completed initial work on this new test. In less than three
weeks, Jenkins’ team both completed the enzyme-linked
immunosorbent assay, or ELISA, that allowed for detection
of COVID-19 antibodies, as well as tested its accuracy.
Fang Li, associate professor in the Department of
Veterinary and Biomedical Sciences, was among the first
to publish a peer-reviewed article detailing the underlying
structure of COVID-19. Li provided protein material to the
Jenkins Lab, and by April 9, with the U of M’s Advanced
Research and Diagnostic Lab led by Amy Karger, M.D., the
test was further validated.
“What makes this test different is that it was developed
here in Minnesota, meaning we aren’t relying on an outside
supply chain for kit parts from another part of the world,”
said Tim Schacker, M.D., vice dean for research at the medical school. “That’s important because we have more control
over the process and can more easily deploy testing where
it is most needed.”
On April 22, Gov. Tim Walz announced the state would allocate $36 million to the medical school and the Mayo Clinic in support of a plan to begin testing 20,000 Minnesotans a day, starting with those who are symptomatic.